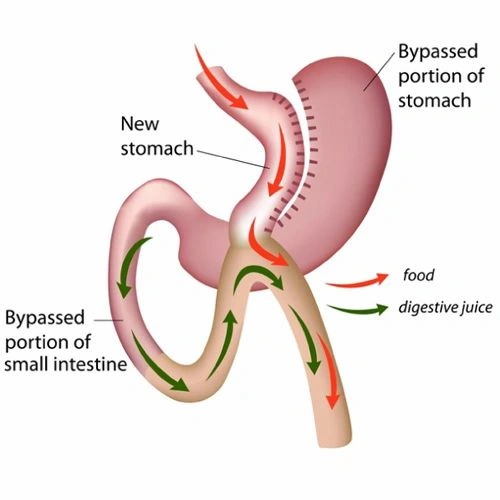
During an OAGB procedure, the surgeon first reduces the size of the “functional” stomach by separating a tubular gastric pouch from the rest of the stomach. This tubular gastric pouch is connected (anastomosed) to the intestine, bypassing up to 200 cm of the upper intestine. This technique differs from the traditional Roux-en-Y bypass (RYGB), which requires two connections (anastomoses).
An OAGB typically results in a 30-40% body weight loss from baseline (60-80% excess weight loss). The most rapid weight loss occurs in the first 6 months after surgery and then continues at a slower rate for another 18 months. This weight loss is achieved through both restriction (the new gastric pouch can hold only a small amount of food) and malabsorption. Bypassing a sizable segment of intestine, the remaining intestine is not long enough for normal nutrient absorption, leading to malabsorption. Substantial weight loss can lead to dramatic improvement and even complete remission of many obesity-related comorbidities. Long-term data show that OAGB may result in slightly greater weight loss and better diabetes resolution than RYGB. The superior diabetes remission rate in OAGB could be attributed to both the greater weight loss and the longer bypassed limb.